


Bipolar affective disorder
Bipolar affective disorder (BPAD) is a mental disorder characterised by alternating symptoms of depression and mania. It affects approximately 2-5% of the population. Usually the first symptoms appear between the ages of 20 and 30. The treatment of bipolar affective disorder is a long-term process, but it contributes significantly to improving the functioning of the patient. This disorder occurs with equal frequency in men and women.
What is bipolar affective disorder (BPAD)?
Bipolar affective disorder is a mental disorder classified as a mood disorder. Despite its name, it is not counted as a mental illness according to the most recent classification. It is characterised by episodes of depressed and elevated (or irritable) mood. States of depression, hypomania (a milder form of mania) and mania usually occur alternately. Usually the depressive episode lasts longer, but the mania episode is the most severe and distressing for people around.
In some cases, so-called mixed episodes may appear characterised by the occurrence of mania and depression at the same time. Mood swings lead to significant impairment in many areas of life. The episodes of mania and depression are followed by a period of remission, when symptoms do not show up or are only mild.
Bipolar affective disorder can vary in its course. For this reason, different types of this disorder have been distinguished, such as:
- Type I – characterised by a severe course, during which both depressive and mania states are very severe;
- Type II – in which depressive episodes are severe, while manias are usually mild (hypomania) and of relatively short duration;
- Rapid Cycling BPAD – characterised by four or more episodes of depression or mania over the course of a year with short or no periods of remission;
- Ultra-Rapid Cycling BPAD – with more frequent phase changes and shorter duration of individual phases;
- Seasonal Affective Disorder – in which periods of depression occur in autumn and episodes of mania in spring and summer.
Symptoms of bipolar affective disorder
Due to the alternation of two mental states in the course of bipolar affective disorder – episodes of depression and mania – its symptoms will vary depending on the current condition.
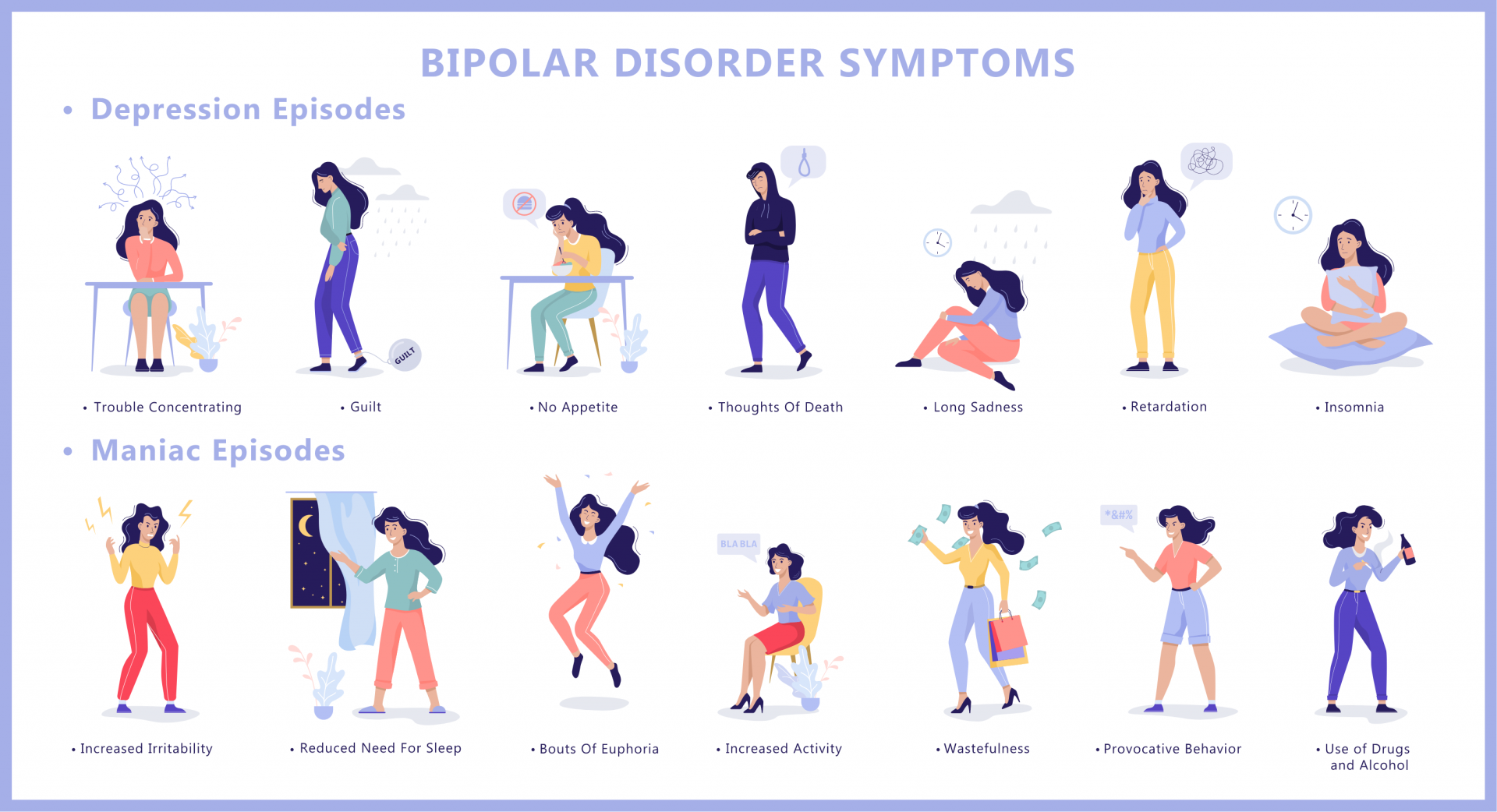
Symptoms of a depressive episode:
- psychomotor retardation and psychomotor disturbances,
- noticeable mood lowering,
- feelings of guilt,
- lowered self-esteem,
- constant feeling of sleepiness, despite getting enough sleep,
- overeating,
- difficulty focusing and concentrating,
- difficulty making decisions,
- difficulties in everyday social and professional functioning,
- racing thoughts,
- emotional lability.
Symptoms of a manic episode:
- increased psychomotor activity,
- insomnia,
- excessive sexual arousal,
- tendency to risky behaviour (risky sexual behaviour, fast driving, taking loans, using psychoactive substances),
- loss of inhibitions,
- increased self-esteem,
- increased self-worth,
- excessive feelings of happiness and joy,
- uncritical attitude to one's own ideas,
- feeling of omnipotence.
Causes of bipolar affective disorder
The causes of bipolar affective disorder are not fully understood. Research suggests that genetic factors play an important role in the pathogenesis of this condition. The risk of developing bipolar affective disorder is five times higher in families with a previous history of BPAD. It is important to note that genetic factors are only a predisposition to the occurrence of bipolar affective disorder. Psychological, environmental and social factors are also important contributors to BPAD. There is a theory that childhood traumas can induce the onset of this disorder.
Relationships with other people, life situations and daily routines may exacerbate or reduce the symptoms of bipolar affective disorder.
How is bipolar affective disorder diagnosed?
Bipolar affective disorder is diagnosed based on the medical history and observation of the clinical picture. Patients usually come to see a psychiatrist in a depressive state, so it is often possible to fully diagnose BPAD only after prolonged observation when the first episode of mania or hypomania occurs.
For a diagnosis of bipolar affective disorder to be made, there must be at least two episodes of clearly disturbed mood and activity, of which at least one must be a manic episode (should last at least 7 days according to the classification), a hypomanic episode (should last up to 4 days) or a mixed episode (should last at least 2 weeks). The symptoms that occur cannot be the result of psychoactive substance use.
How is bipolar affective disorder treated?
Treatment for bipolar affective disorder usually involves a combination of pharmacological therapy and psychotherapy. The treatment strictly depends on the course of the disorder and its current phase.
The first-line drugs used to treat bipolar affective disorder are often normothymic drugs, or so-called mood stabilisers. The most commonly used medications are: lithium salts, carbamazepine and valproic acid. In some cases, atypical neuroleptics have proven effective in reducing symptoms of mania.
Treatment of depression in bipolar affective disorder is extremely difficult. Depression in BPAD tends to be more severe than recurrent depression. Medication for bipolar depression should be administered with great care, because depression often tends to progress to mania as a consequence of medication. Usually monotherapy is not used, only antidepressants combined with mood stabilisers.
While treating affective disorder, participation in psychotherapy is extremely important. The most common form is cognitive behavioural psychotherapy. It supports pharmacological treatment and reduces the intensity and duration of episodes of mania and depression. Psychotherapy also helps to understand bipolar affective disorder, to raise awareness of BPAD, and thus to effectively improve well-being of the patient.
All of the above treatment modalities result in significant improvements in the patient’s functioning. Although bipolar affective disorder has a severe course and often causes distress to the patient, with appropriate treatment the prognosis of bipolar affective disorder is positive.
opracowanie
mgr Barbara Wróblewska
Poleska J. (2018). Od depresji do manii – choroba afektywna dwubiegunowa
Gorostowicz A., Siwek M. (2018). Trudności w diagnostyce choroby afektywnej dwubiegunowej